 On August 6th, a school board in Mt. Vernon Indiana heard some interesting testimony regarding COVID-19 and vaccines from Dr. Dan Stock, a McCordsville resident and family medicine physician (Link). Since our own boys are headed back to school shortly, it’s no wonder that many have sent me this video asking me my opinion on Stock’s presentation.
On August 6th, a school board in Mt. Vernon Indiana heard some interesting testimony regarding COVID-19 and vaccines from Dr. Dan Stock, a McCordsville resident and family medicine physician (Link). Since our own boys are headed back to school shortly, it’s no wonder that many have sent me this video asking me my opinion on Stock’s presentation.
Table of Contents
- 1 Facemasks ineffective:
- 2 Animals reservoirs:
- 3 Antibody-Dependent Viral Enhancement:
- 4 More vaccinated rather than unvaccinated people getting infected:
- 5 Vitamin D:
- 6 Ivermectin:
- 7 Those previously infected gain nothing from vaccines:
- 8 More than 96% of Doctors are Fully Vaccinated:
- 9 Review by Dr. Zubin Damania:
- 10 Delta Variant: Top 10 COVID Questions and How to Prepare:
- 11 Dr. Sean Pitman:
Facemasks ineffective:
 Dr. Stock starts off by claiming that the COVID-19 virus is far too small for masks to even slow them down.
Dr. Stock starts off by claiming that the COVID-19 virus is far too small for masks to even slow them down.
Now, while it may seem difficult to see how facemasks in a grade school setting would provide very much benefit, children being children and all, the latest data appears to support the conclusion that masks in schools do in fact reduce the transmission rates of COVID-19.
In some places where schools have been open for a while now, such as Georgia and Hawaii, public health experts notice what happens when schools follow the science: classes go on without disruption as long staff and students wear masks.

Also, Dr. Stock is not technically correct when he says that masks cannot work because the virus is so small that they would fly right through any mask one might wear. SARS-CoV-2 is an enveloped virus ~0.1 μm in diameter. The length of rod- or filament-shaped viruses can measure to as long as 1 μm. (Link). In comparison, reusable surgical-type masks have pore diameters ranging from 20 to 100 µm, whereas N95 masks have pore diameters ranging from 10 to 65 µm (Link). So, it would seem reasonable that using masks to stop the COVID-19 virus would be about as reasonable as using a chicken-wire fence to stop mosquitoes.
The problem with this particular argument is that respiratory viruses, COVID-19 in particular, are not transmitted in infectious doses via individual viruses flying independently through the air. Rather, they are transmitted within respiratory droplets and aerosols, sometimes in large numbers within these droplets, and are then inhaled into the nasopharynx and respiratory passages of others in the vicinity. It is for this reason that face-masks (surgical types and even many cloth types) do reduce the number of infected respiratory droplets that are given off by an infected person, and even reduce the number of these infected droplets that are inhaled by someone wearing a mask (although reduction of transmission appears to be the prime benefit for mask-wearing in public places). Also, the nano fabrics of face masks such as surgical and N95 masks, will be given an electrostatic charge to enhance the small particle capture ability (Link).
No one is saying that masks are perfect – not even N95 masks block all aerosols that may contain viruses. What is being said is that masks reduce, but do not completely eliminate, the spread of respiratory droplets and aerosols – thereby reducing, but not eliminating, the number of viruses transmitted from one mask-wearing person to another mask-wearing person within a given span of time. Masks also reduce the forward speed of airflow and therefore the speed of the aerosols leaving the mouth/nose of a person. You can’t even blow out a candle at 2 inches with a surgical mask on.
Multi-layer cloth masks block release of exhaled respiratory particles into the environment, along with the microorganisms these particles carry. Cloth masks not only effectively block most large droplets (i.e., 20-30 microns and larger) but they can also block the exhalation of fine droplets and particles (also often referred to as aerosols) smaller than 10 microns; which increase in number with the volume of speech and specific types of phonation. Multi-layer cloth masks can both block up to 50-70% of these fine droplets and particles and limit the forward spread of those that are not captured. Upwards of 80% blockage has been achieved in human experiments that have measured blocking of all respiratory droplets, with cloth masks in some studies performing on par with surgical masks as barriers for source control. (CDC, May 7, 2021)
.
Both surgical masks and unvented KN95 respirators, even without fit-testing, reduce the outward particle emission rates by 90% and 74% on average during speaking and coughing, respectively, compared to wearing no mask, corroborating their effectiveness at reducing outward emission. (Asadi, et. al., September 24, 2020)
N95 masks are designed to remove more than 95% of all particles that are at least 0.3 microns (µm) in diameter. In fact, measurements of the particle filtration efficiency of N95 masks show that they are capable of filtering ≈99.8% of particles with a diameter of ≈0.1 μm (Rengasamy et al., 2017).
Again, while certainly not perfect, not by a long shot, masks are better than nothing. Of course, now that we have the mRNA vaccines, these vaccines are far more effective compared to masks – make no mistake about it!
So, while it may be tempting to conclude that masks in a grade school setting probably have limited practical value for numerous reasons, the reasons given by Dr. Stock here aren’t technically correct and the actual observations of masks in action do seem to have actual real-world benefits – even in the grade-school setting.

Dr. Anthony Kaveh, August 24, 2020
Animals reservoirs:
 Animals reservoirs are a problem for the flu virus and other such respiratory viruses. However, I’m not aware of a significant animal reservoir for COVID-19. It’s a real and serious possibility, however, since SARS-CoV-2 has been transmitted to various animals and there have been cases of animal to human transmission (Link).
Animals reservoirs are a problem for the flu virus and other such respiratory viruses. However, I’m not aware of a significant animal reservoir for COVID-19. It’s a real and serious possibility, however, since SARS-CoV-2 has been transmitted to various animals and there have been cases of animal to human transmission (Link).
Antibody-Dependent Viral Enhancement:
 Dr. Stock is seriously mistaken, however, about antibody-dependent viral enhancement. The mRNA vaccines were specifically designed to avoid this particular problem.
Dr. Stock is seriously mistaken, however, about antibody-dependent viral enhancement. The mRNA vaccines were specifically designed to avoid this particular problem.
There is a very real concern for antibody-dependent enhancement (or ADE) when developing any new vaccine – where the vaccine can result in the production of antibodies that make an infection worse rather than effectively fight against it. This concern was front and center for the development of the vaccines against COVID-19 as well – that the ADE problem could be overcome. And, the ADE problem was overcome for the vaccines against COVID-19 (Link).

More vaccinated rather than unvaccinated people getting infected:
 But what about Dr. Stock’s claims regarding the evidence that even those who are vaccinated still get infected by COVID-19? – particularly the delta variant? As an example of this, consider a series of large public events that occurred over several days in Cape Cod, Massachusetts (from July 3–17). This “event” or “series of events” if you prefer, resulted in 469 people being infected with Covid-19 (as initially reported by the CDC). Of this number, 346 (74%) occurred in fully vaccinated persons! Most cases occurred in males (85%) with a median age was 40 years. Five were hospitalized and no deaths were reported. One hospitalized patient (age range = 50–59 years) was not vaccinated and had multiple underlying medical conditions. Four additional fully vaccinated patients (aged 20–70 years) were also hospitalized, two of whom had underlying medical conditions. Initial genomic sequencing of specimens from 133 patients identified the Delta Variant in 119 (89%) cases and the Delta AY.3 sublineage in one (1%) case (Link).
But what about Dr. Stock’s claims regarding the evidence that even those who are vaccinated still get infected by COVID-19? – particularly the delta variant? As an example of this, consider a series of large public events that occurred over several days in Cape Cod, Massachusetts (from July 3–17). This “event” or “series of events” if you prefer, resulted in 469 people being infected with Covid-19 (as initially reported by the CDC). Of this number, 346 (74%) occurred in fully vaccinated persons! Most cases occurred in males (85%) with a median age was 40 years. Five were hospitalized and no deaths were reported. One hospitalized patient (age range = 50–59 years) was not vaccinated and had multiple underlying medical conditions. Four additional fully vaccinated patients (aged 20–70 years) were also hospitalized, two of whom had underlying medical conditions. Initial genomic sequencing of specimens from 133 patients identified the Delta Variant in 119 (89%) cases and the Delta AY.3 sublineage in one (1%) case (Link).
That sounds like a problem until one realizes that 72% of the population in Massachusetts has received at least one vaccine dose, and, overall, 4,389,137 people or 63% of Massachusetts’s population has been fully vaccinated. Of those 75 years of age and older, the rate of full vaccination is 81.7% and for those 50-74 years of age, the rate of full vaccination in this state is over 80%. And, the vaccine rate is even high for those who are in their 20s, 30s, and 40s in this region (Link). Only the children have a low rate of vaccination because the vaccines are not available to children yet. And, those attending these large events were supposed to be vaccinated.
Clearly, then, as in the UK, the significant majority of those older than 30 years of age have been fully vaccinated. So, it only stands to reason that the majority of infections, and even deaths (particularly in the UK), would be among those who have been vaccinated since the effectiveness of the vaccines is not 100%. It’s very good, but not 100%. When it comes to the original type of COVID-19, vaccines not only provide significant protection against hospitalization and death, but also significantly reduce the transmission rate of the virus to others.
 What is different, then, about this Massachusetts data, is that the delta variant seems to have a much higher infection rate, even among those who have been vaccinated, as compared to the original COVID-19 virus of 2020. Just watch the video of well-known and well-respected pulmonologist Dr. Roger Seheult where he explains that the only group of people that has a decreased risk of severe infection requiring hospitalization and/or death from the Delta Variant is not the unvaccinated group, or even the partially vaccinated group, but the fully vaccinated group (within a particular age category): Link
What is different, then, about this Massachusetts data, is that the delta variant seems to have a much higher infection rate, even among those who have been vaccinated, as compared to the original COVID-19 virus of 2020. Just watch the video of well-known and well-respected pulmonologist Dr. Roger Seheult where he explains that the only group of people that has a decreased risk of severe infection requiring hospitalization and/or death from the Delta Variant is not the unvaccinated group, or even the partially vaccinated group, but the fully vaccinated group (within a particular age category): Link
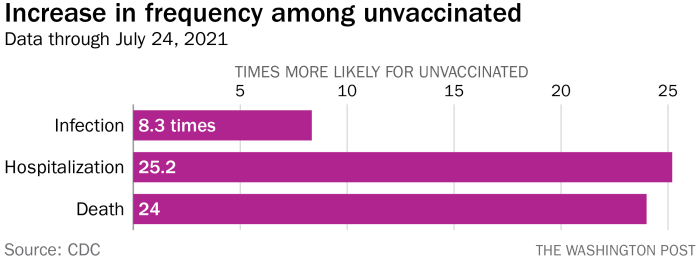
Again, when it comes to the severity of illness and deaths, all of the data worldwide, the UK data included, strongly supports the conclusion that the unvaccinated, within a particular age category, are at a far far higher risk of hospitalization and death from COVID-19 infections (particularly the delta variant now) as compared to those who are fully vaccinated against COVID-19 – via the mRNA vaccines in particular. More than 99% of those who are dying of COVID-19 right now, within a particular age category, are the unvaccinated – in this country and around the world (Link, Link). The unvaccinated also have a much higher hospitalization rate.
Sure, the Delta Variant of COVID-19 has reduced the ability of the current mRNA vaccines to make someone resistant to infection. However, recent research still shows relatively substantial protection for those who are fully vaccinated relative to those who are not vaccinated. Consider, for example, the results of the Imperial-led REACT-1 study based on swab tests taken by almost 100,000 people in England between 24 June and 12 July, 2021 – specifically dealing with the Delta Variant of COVID-19 (Link):
“Fully vaccinated people… had around a 50% to 60% reduced risk of infection, including asymptomatic infection, compared to unvaccinated people. In addition, double vaccinated people were less likely than unvaccinated people to test positive after coming into contact with someone who had COVID-19 (3.84% vs 7.23%)… The study’s… results also suggest that fully vaccinated people may be less likely than unvaccinated people to pass the virus on to others, due to having a smaller viral load on average and therefore likely shedding less virus.”
This is on top of the dramatically reduced risks of hospitalization and death for those who are fully vaccinated (more than 95% of those who are being hospitalized and/or dying of COVID-19 right now, within a given age range, are unvaccinated).
Key Facts from the REACT Study:
- Three times as many unvaccinated people tested positive for Covid-19 than those who had been fully vaccinated, the REACT study found, with all positive samples analyzed indicating an infection with the delta Covid-19 variant.
- Once other factors are taken into account, the study, which is based on data from over 98,000 swab tests taken between June 24 and July 12 and has not yet been peer reviewed, indicates full vaccination halves the risk of catching Covid-19 caused by the delta variant.
- Fully vaccinated people who were infected with the virus tended to have less severe illness than unvaccinated people and seemed to have smaller amounts of virus in samples, the researchers added, meaning they may be less likely to pass it on if they are infected.
- Professor Paul Elliott, director of the research program running the study, said the findings confirm “previous data showing that both doses of a vaccine offer good protection against getting infected,” but show there “is still a risk of infection among the fully vaccinated.”
- The researchers estimated that two doses of a Covid-19 vaccine are 49% effective at preventing infection with the delta variant, in line with recent data from Israel and much lower than previous estimates.
- “Development of vaccines against delta may be warranted” given the reduced effectiveness of current vaccines against the strain, the researchers wrote, warning that even high levels of vaccination may be unable to stop it spreading in the fall.
Robert Hart, Forbes.com, August 4, 2021
So, not only is it very advantageous to a particular person to get fully vaccinated against COVID-19, even when it comes to the current “variants of interest”, such as the Delta Variant, in particular, it also appears to be helpful in reducing the transmission of COVID-19 and it’s current variants. I’d call that very “effective” – and so would the vast majority of doctors and medical scientists. Of course, if your definition of “effective” is absolute perfection, well, you’ll be waiting a while for sure. Until then, I would strongly advise you and everyone else who has access to get fully vaccinated as soon as possible.

Vitamin D:
 Also, while I’m a big fan of vitamin D, it’s just not enough to deal effectively with a virus as infectious as the Delta Variant of COVID-19. Sure, various studies have shown that those who are deficient in Vitamin D can gain substantial advantages when it comes to resisting various viral infections if they start improving their Vitamin D levels. If everyone in this country had adequate levels of Vitamin D on board (> 50 ng/mL), then perhaps the overall death rate would have been reduced by more than half – no exaggeration since most people are Vitamin D deficient. However, compared to the effectiveness of the mRNA vaccines (more than 95% reduction in hospitalizations and deaths, and an 8 fold reduction in infection rates, and therefore transmissibility), this isn’t remotely good enough.
Also, while I’m a big fan of vitamin D, it’s just not enough to deal effectively with a virus as infectious as the Delta Variant of COVID-19. Sure, various studies have shown that those who are deficient in Vitamin D can gain substantial advantages when it comes to resisting various viral infections if they start improving their Vitamin D levels. If everyone in this country had adequate levels of Vitamin D on board (> 50 ng/mL), then perhaps the overall death rate would have been reduced by more than half – no exaggeration since most people are Vitamin D deficient. However, compared to the effectiveness of the mRNA vaccines (more than 95% reduction in hospitalizations and deaths, and an 8 fold reduction in infection rates, and therefore transmissibility), this isn’t remotely good enough.
Ivermectin:
 As far as Ivermectin is concerned, also promoted by Dr. Stock, I really wished it worked, but multiple studies have not been able to demonstrate more than modest benefits against COVID-19 – so far. (Link, Link)
As far as Ivermectin is concerned, also promoted by Dr. Stock, I really wished it worked, but multiple studies have not been able to demonstrate more than modest benefits against COVID-19 – so far. (Link, Link)
Those previously infected gain nothing from vaccines:
 Stock’s claim that those who have previously recovered from a COVID-19 infection get no additional benefit now that they’ve gained natural immunity, from vaccines, actually seems to be supported by the most resent scientific research coming out of Israel.
Stock’s claim that those who have previously recovered from a COVID-19 infection get no additional benefit now that they’ve gained natural immunity, from vaccines, actually seems to be supported by the most resent scientific research coming out of Israel.
This analysis demonstrated that natural immunity affords longer lasting and stronger protection against infection, symptomatic disease and hospitalization due to the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity. Notably, individuals who were previously infected with SARS-CoV-2 and given a single dose of the BNT162b2 vaccine gained additional protection against the Delta variant. (Gazit, et. al., August 25, 2021)
.Sivan Gazit is a physician and researcher, deputy managing director of KSM Research and Innovation Center at Maccabi Healthcare Services..
The natural immune protection that develops after a SARS-CoV-2 infection offers considerably more of a shield against the Delta variant of the pandemic coronavirus than two doses of the Pfizer-BioNTech vaccine, according to a large Israeli study that some scientists wish came with a “Don’t try this at home” label. The newly released data show people who once had a SARS-CoV-2 infection were much less likely than vaccinated people to get Delta, develop symptoms from it, or become hospitalized with serious COVID-19.
The study demonstrates the power of the human immune system, but infectious disease experts emphasized that this vaccine and others for COVID-19 nonetheless remain highly protective against severe disease and death. And they caution that intentional infection among unvaccinated people would be extremely risky. “What we don’t want people to say is: ‘All right, I should go out and get infected, I should have an infection party.'” says Michel Nussenzweig, an immunologist at Rockefeller University who researches the immune response to SARS-CoV-2 and was not involved in the study. “Because somebody could die.”..
“These results suggest that boosting vaccinated individuals with currently available mRNA vaccines would produce a quantitative increase in plasma neutralizing activity but not the qualitative advantage against variants obtained by vaccinating convalescent individuals.”.
More than 96% of Doctors are Fully Vaccinated:
According to a recent AMA survey (June 11, 2021) more than 96% of doctors in this country are now fully vaccinated with another 2% soon to be fully vaccinated – for a total of 98%.
“Practicing physicians across the country are leading by example, with an amazing uptake of the COVID-19 vaccines,” said AMA President Susan R. Bailey, MD. “Physicians and clinicians are uniquely positioned to listen to and validate patient concerns, and one of the most powerful anecdotes a physician can offer is that they themselves have been vaccinated. You can take it from your doctor: the COVID-19 vaccines are safe and effective. With COVID-19 vaccines readily available and approved for all people 12 years old and up, we urge you to get vaccinated—take the single most important step you can to protect yourself, your family, and end the COVID-19 pandemic.” (Link)
Highest level of Vaccine Hesitancy among those with a Ph.D.:
In contrast, however, is the increased vaccine hesitancy among those with Ph.Ds. It might sound surprising, but, apparently, the two groups with the highest levels of those with vaccine hesitancy are those with only a high school level of education, or less – and those with a Ph.D. (Link)

56 This analysis used the COVID Trends and Impact Survey (CTIS), created by the Delphi Group at 57 Carnegie Mellon University (CMU) and conducted in collaboration with Facebook Data for 58 Good. Survey sampling is described in the eMethods. Survey weights accounting for the 59 sampling design and non-response are post-stratified to match the US general population by 60 age, gender, and state. The study design ensures CMU researchers do not see usernames or 61 profile information and Facebook does not see survey microdata. Link
Another concept to remember here is that a Ph.D. can be in “molecular biology just as much as it can be in comparative linguistics.” In other words, just because one has a Ph.D. in something doesn’t mean that this increases a person’s ability to understand the medical science involved with viruses or vaccines.
Review by Dr. Zubin Damania:
Delta Variant: Top 10 COVID Questions and How to Prepare:
Dr. Sean Pitman:
_____________
 Dr. Sean Pitman is a pathologist, with subspecialties in anatomic, clinical, and hematopathology, currently working in N. California.
Dr. Sean Pitman is a pathologist, with subspecialties in anatomic, clinical, and hematopathology, currently working in N. California.








